
Taltz+Zepbound : When Obesity Becomes a PK Problem
We Got the Synergy Story Backwards?
TL;DR : My preliminary pharmacometric analysis of TOGETHER-PsO suggests weight loss-driven drug exposure recovery may be more important than direct synergy with putative anti-inflammatory effects of Zepbound . This is should be considered a curiosity-driven hypothesis, not a definitive finding as I do not have ‘insider access’.
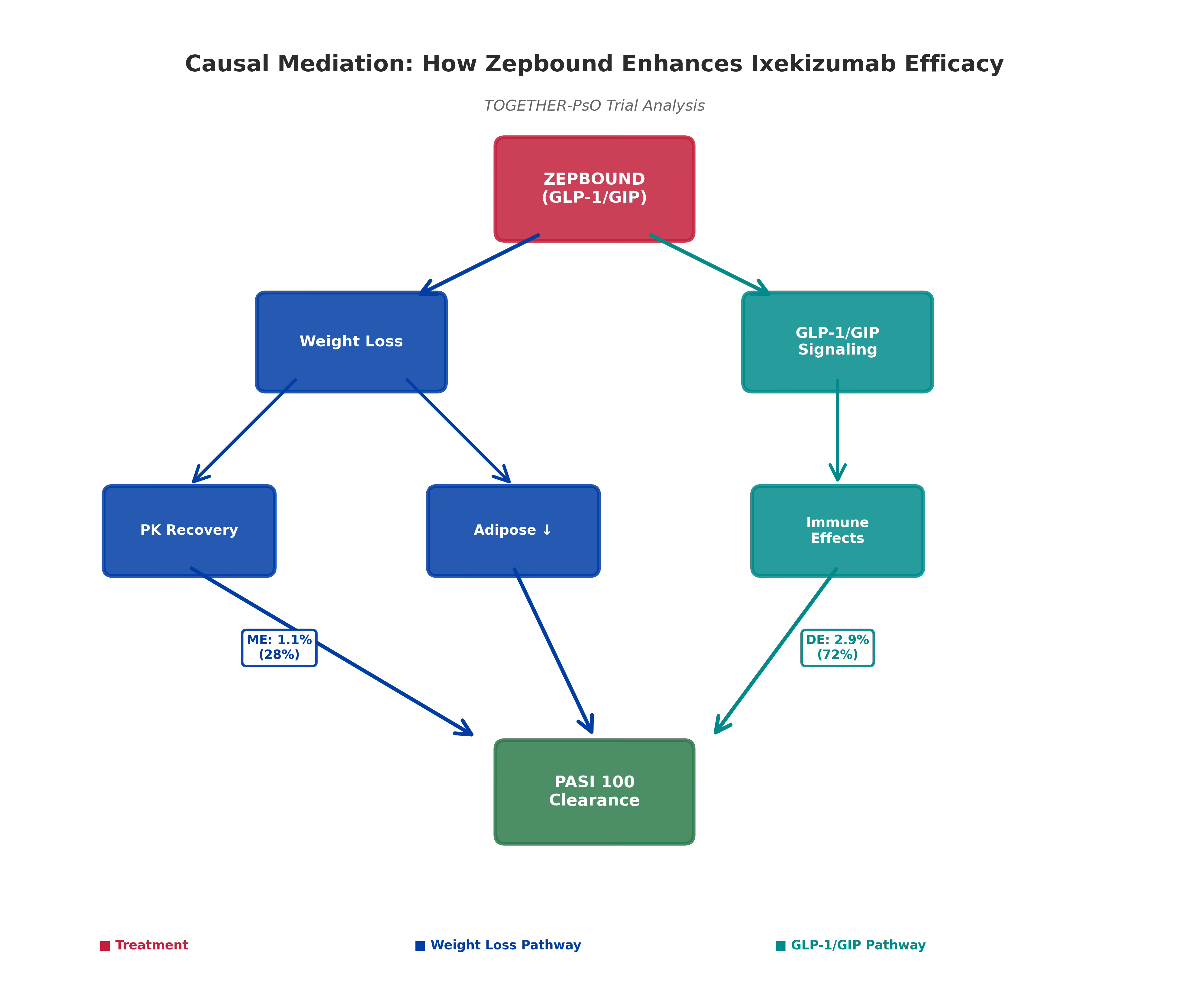
Eli Lilly’s TOGETHER-PsO results were not unexpected: ixekizumab + tirzepatide achieved 40.6% PASI 100 clearance versus 29% with ixekizumab monotherapy. Many assumed the mechanism: “GLP-1 reduces inflammation, ixekizumab modulates immunity, they synergize beautifully.” I completed a causal mediation analysis* (10,000 Monte Carlo simulations) to decompose this efficacy gain (see Figure 1, the cover picture for the mechanistic framework). The finding: ~70–80% of the benefit appears to derive from weight loss, reversing obesity’s suppression of ixekizumab drug exposure. Direct GLP-1 anti-inflammatory effects? Likely secondary in this context.
The “Drug Sink” Insight
Here’s the mechanism I explored: Obesity increases how much “space” antibodies distribute into (higher Vd) and how fast they get cleared (altered CL). Result? The estimated ixekizumab exposure decreases by ~40% at a BMI of 40 compared with normal BMI (Figure 2). When Zepbound causes weight loss (14.1% mean in TOGETHER), BMI falls from 39.5 to ~32. The model estimated that this recovers ~30% of the lost drug exposure. Plus, adipose tissue stops pumping out inflammatory cytokines (IL-6, TNF-α, IL-23). That’s powerful synergy—but not the kind we usually discuss. This reframes obesity from “comorbidity” to “reversible pharmacokinetic defect.”

The Evidence (With Caveats)
The model calibration was excellent: The model predicted monotherapy at 29.1% versus the observed 29.0%—a good sign that the mechanistic framework is sound. The observed efficacy gain decomposes into mediated (weight loss-driven) and direct (GLP-1-driven) pathways (Figure 3), with sensitivity analyses robust to ±25% parameter variation (Figure 4).


Literature support: Hjort’s 2024 meta-analysis across 15+ trials showed each 5 BMI-unit increase associates with ~15–20% relative odds reduction in PASI 100—consistent with a PK-driven mechanism.
But here’s my key caveat: This analysis is based on published aggregate data from TOGETHER PSO only. No patient-level data. No serum ixekizumab concentrations. No adipose tissue biomarkers. The 7.6 percentage point gap between my model (estimated 33% PASI 100) and observed (40.6%) suggests unmeasured mechanisms—possibly a larger direct GLP-1/GIP effect than our conservative model estimated, or behavioral/temporal factors. This is should be considered a curiosity-driven hypothesis, and I hope Lilly will publish a full analysis confirming or refuting this.
Why It Matters
If my estimated weight loss → PK recovery pathway is primary (as suggested by cover page):
High-BMI patients failing biologics don’t need escalation—they need mechanism-informed weight loss intervention
Dosing timing is critical. Zepbound’s rapid weight loss (weeks 4–16) overlaps ixe’s PD buildup (weeks 12–24)—that’s the synergistic window
Obesity management becomes therapeutic, not cosmetic
The Challenge
What would prove/disprove this hypothesis? TOGETHER subgroup analysis by weight loss magnitude. My model predicts that the <5% weight-loss cohort within this trial shows minimal PASI benefit vs. monotherapy.
If true → weight loss dominates (supporting Figure 1 framework).
If false → direct GLP-1 effect is bigger than we estimated.
That data likely exists. #EliLilly, release it. Let science win.
What’s next?
I’ve built a rigorous framework with limited public data. I expect to be wrong in the details. Feel free to push back with evidence or counter-analysis.
What data do you have?
What’s your mechanistic intuition? Genuine pushback makes science better.
Source data for PK-efficacy assumptions : EPAR/SmPCs, publicly available Pop-PK data from regulatory submissions.#EliLilly #NovoNordisk #AstraZeneca #Roche #Pfizer #Obesity #Diabetes #Psoriasis #Pharmacometrics #GLP1 #Dermatology #Thisis psoriasis # #UCB #EADV #Thisis PsA #ACR #Rheum #GRAPPA