
Inflammatory Hand Osteoarthritis is a Critical Unmet Medical Need
What do we drug developers need to do?

Let's start with a working definition: an unmet medical need describes a situation where no satisfactory method of diagnosis, prevention, or treatment exists for a condition. Or, if such methods do exist, a new approach would offer a significant therapeutic advantage. This perfectly encapsulates the current state of hand osteoarthritis (HOA), a common and debilitating condition that cries out for innovation.
Hand Osteoarthritis: A Pervasive and Burdensome Condition
Hand osteoarthritis is far from a rare ailment. It's a chronic, disabling disease with a staggering lifetime risk of up to 40%. Globally, osteoarthritis affects over 500 million people, and hand OA is a significant contributor to this burden, accounting for nearly a quarter of all disability-adjusted life years (DALYs) attributed to osteoarthritis – second only to knee OA. The Global Burden of Disease study (1990-2019) highlighted that in 2019 alone, there were 1.53 million new cases of HOA, with an overall prevalence of 159.46 million cases worldwide. This translates to millions of individuals experiencing persistent pain, stiffness, reduced grip strength, and significant difficulties with everyday fine motor tasks. The impact on quality of life is profound, and the economic burden, while not often singled out for HOA specifically, is substantial when considering osteoarthritis as a whole, costing an estimated 1-2.5% of the gross national product in established market economies.
The Elephant in the Joint: Inflammation and Synovitis
For too long, osteoarthritis was dismissed as a simple "wear and tear" disease, a non-inflammatory condition distinct from diseases like rheumatoid arthritis. However, this view is outdated. Strong evidence now clearly indicates that synovial inflammation (synovitis) is not just present but common in osteoarthritis, playing a crucial role in both symptoms and disease progression. Observational studies specifically on hand OA have consistently shown that synovitis is common and is associated with both pain and the worsening of the disease. In most hospital-based hand osteoarthritis (OA) studies, the majority of participants exhibit evidence of synovitis in at least one hand joint when examined by MRI or ultrasound. For instance, in the Nor-Hand study, about two-thirds of participants had synovitis in their interphalangeal joints, and one-third had it in their thumb carpometacarpal joint.
This inflammation isn't a silent bystander. While the total amount of synovitis across the whole hand might only weakly correlate with overall hand pain, synovitis in an individual joint is strongly associated with pain in that specific joint. This link has been confirmed in finger joints. Furthermore, a relationship between synovitis and future disease progression, including the development of erosions, has been demonstrated in multiple hand OA cohorts. This mirrors findings in knee OA, where synovitis is also linked to pain and disease progression. The inflamed synovium in osteoarthritis (OA) joints is characterized by an immune response dominated by the innate immune system, with macrophages playing a crucial role. This inflammatory milieu leads to the release of various mediators, including cytokines like TNF-α, IL-1β, and IL-6, which contribute to pain by sensitizing nociceptors and drive cartilage degradation and bone remodeling. See Table 1
Table 1: Key Inflammatory Mediators and Pathways Implicated in Hand Osteoarthritis Pathogenesis
Proving the Unmet Need: Where Current Treatments Fall Short
Given the prevalence, burden, and the clear role of inflammation, especially synovitis, in driving pain and progression in HOA, one would expect a plethora of effective, targeted treatments. Sadly, this is not the case. Current treatments for HOA are largely symptomatic and fail to address the underlying disease processes, particularly inflammation, in a meaningful or sustained way. This gap firmly establishes HOA as an unmet medical need.
Let's look at the limitations of existing therapies (See Table 2):
Table 2: Limitations of Current Pharmacological Treatments for Hand Osteoarthritis
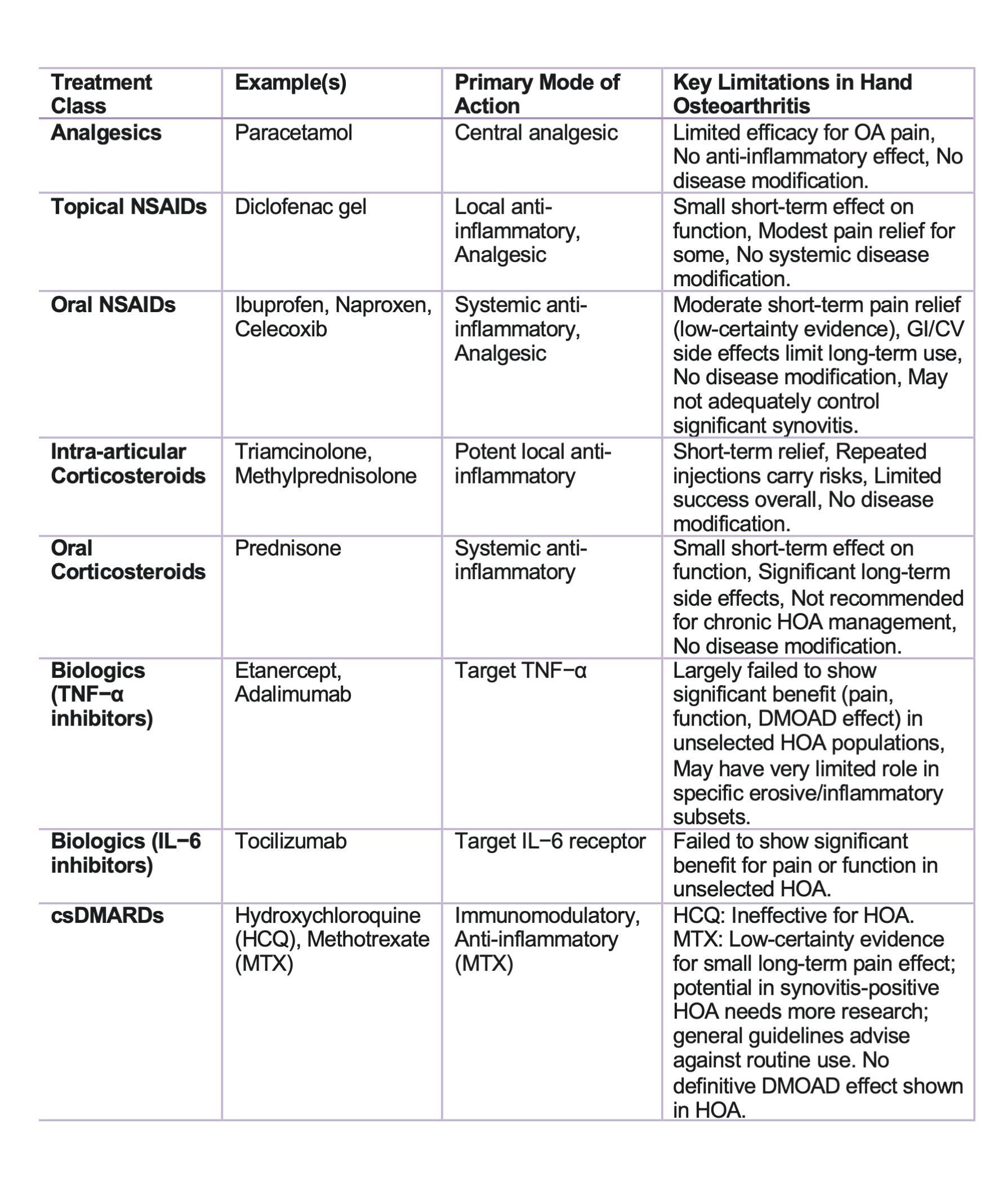
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs):
Topical NSAIDs: Recommended as a first-line pharmacological treatment by EULAR due to a favorable safety profile. However, supporting evidence is limited, with only one high-quality placebo-controlled trial and conflicting results from studies comparing them to other interventions. Their practicality is also questioned due to the need for frequent hand washing. As of February 2025, no ongoing placebo-controlled randomized controlled trials (RCTs) investigating topical non-steroidal anti-inflammatory drugs (NSAIDs) in hand osteoarthritis (OA) were listed on clinicaltrials.gov, highlighting a significant research gap.
Oral NSAIDs: Have demonstrated moderate efficacy in reducing short-term pain. However, their use is limited by potential systemic side effects, especially with long-term use, making them unsuitable as a chronic solution.
Corticosteroids: These are potent anti-inflammatory drugs.
Oral Corticosteroids: The HOPE study demonstrated that 10 mg of prednisolone administered daily significantly reduced pain and improved symptoms in hand osteoarthritis (OA) after six weeks, supporting the hypothesis that synovitis is a key contributor to pain. Treatment even led to a reduction in ultrasound-defined synovial thickening and MRI-defined bone marrow lesions. However, the benefits waned after treatment discontinuation, and long-term systemic side effects make prednisolone unsuitable for chronic use in HOA, though it may be effective for short-term relief.
Intra-articular Corticosteroid Injections: Frequently used in clinical practice, but supporting evidence mainly comes from knee OA studies, and its applicability to hand OA is uncertain. EULAR guidelines suggest that they may be considered for painful interphalangeal osteoarthritis (OA), but recommend against routine use. Studies on their use in the first carpometacarpal (thumb base) joint have largely failed to show a significant benefit over saline or local anesthesia, although methodological limitations, including small sample sizes and the absence of a baseline synovitis requirement for inclusion, prevent definitive conclusions.
Disease-Modifying Anti-Rheumatic Drugs (DMARDs):
Synthetic DMARDs (sDMARDs):
Hydroxychloroquine: Multiple placebo-controlled RCTs, even in erosive (more inflammatory) hand OA, found no significant benefit, suggesting it's unlikely to have a role in HOA management. The lack of synovitis as an inclusion criterion was a limitation in some earlier studies.
Methotrexate (MTX): Results have been more promising but inconsistent. An open-label study first reported symptomatic improvements. One RCT in erosive HOA showed a non-significant trend towards pain relief with 10 mg/week MTX. However, the METHODS trial, using a higher dose (20 mg/week), demonstrated a statistically significant and clinically relevant reduction in pain after six months in patients with synovitis. The Ferrero et al. study also yielded interesting results, with less erosion development and increased repair in MTX-treated patients, although the METHODS trial did not assess structural progression. Neither prednisolone nor methotrexate is currently recommended in international guidelines for HOA, primarily because the key studies supporting their efficacy were published after the most recent updates to the EULAR and ACR guidelines.
Biological DMARDs (bDMARDs): Despite many trials focusing on hand OA (evaluating TNF inhibitors, IL-1, IL-6, and GM-CSF inhibitors), these have generally not achieved their primary efficacy endpoints. Consequently, current guidelines do not recommend their use. Some analyses suggest potential disease-modifying effects of TNF inhibitors in swollen joints or possible clinical benefits in per-protocol analyses, indicating that the final word on inhibiting these cytokines may not yet be spoken. The failure of these biologics may be due to OA's clinical heterogeneity and the possibility that the inflammatory mechanisms in OA differ from those in diseases like rheumatoid arthritis, where these drugs are effective.
Other Anti-Inflammatory Treatments: Apremilast, colchicine, and diacerein have also been tested against a placebo in hand OA without success.
In essence, there are currently no approved disease-modifying osteoarthritis drugs (DMOADs) for hand osteoarthritis. The existing arsenal primarily offers temporary symptomatic relief with limited efficacy, particularly for the inflammatory component, and often comes with concerns about side effects or practicality. There's a persistent gap between our growing mechanistic understanding of HOA and therapeutic success.
The Market and Commercial Opportunity: A Call for Innovation
The overall osteoarthritis market is substantial and growing, projected to expand significantly in the coming years, driven by aging populations and increasing obesity rates. While specific market size figures for hand OA are often subsumed under the general OA market, the "Erosive Hand Osteoarthritis Market" alone was estimated at USD 3.77 billion in 2025 and is projected to reach USD 6.30 billion by 2032, growing at a CAGR of 7.6%. This highlights a significant commercial opportunity.
The limited effectiveness of current treatments for (erosive) hand OA, which only provide symptomatic relief without altering disease progression, is a key driver for this market. There is a clear need and commercial incentive for novel therapies, particularly DMOADs that target specific underlying pathways of the disease, including inflammation and structural damage. Such drugs could be first-in-class for this debilitating condition. The projected 48.6% increase in hand OA cases by 2050 underscores the growing patient population and, consequently, the expanding market for effective treatments.
Call to action
The evidence is clear: synovitis is a common and crucial factor in the pain and progression of hand osteoarthritis. Yet, our current treatments largely fail to effectively target this inflammation. This glaring unmet medical need demands a shift in focus from drug developers. Future clinical trials must prioritize the careful selection of study populations with clear signs of synovitis and possibly MRI evidence of inflammation, employ appropriate treatment durations, and include long-term follow-up to assess potential disease-modifying effects. It's time to move beyond simply managing symptoms and earnestly pursue therapies that can quell the inflammatory fire in hand osteoarthritis, offering real hope for modifying the disease and improving the lives of millions.