
How Can We Rescue Promising Therapies from Clinical Development's "Valley of Death"?
The key seems to be distinguishing avoidable errors from inevitable risks

The "Valley of Death" (VoD) refers to the critical transitional stage where a drug candidate, having shown promise in in vitro and in vivo preclinical models, enters human clinical trials. It's here, typically during Phase I (safety), Phase II (efficacy and dose-ranging), and early Phase III (larger-scale efficacy and safety), that the highest rates of attrition occur. As one source notes, "The VoD is defined as the transition of a company from pre-clinical stages to human trials, which most efforts do not survive."1 (Rapid Innovation Group). The chasm signifies a gap not just in funding, but in translational predictability, where promising science fails to translate into tangible clinical benefit for patients.
Consider this stark reality: while estimates vary, the overall probability of success from Phase I to approval can be distressingly low. For instance, one analysis highlighted by the NCBI indicates that overall success rates post-Phase I can be as low as 19% for all investigated projects, with specific therapeutic areas, such as oncology, facing even steeper odds (e.g., a 8% likelihood of overall approval from Phase 1 for neoplasms in one academic study cohort).
The journey from lab bench to bedside is arduous. Consider these sobering average success rates in clinical development:
Preclinical to Phase I: ~50-60% (Initial human safety hurdles)
Phase I to Phase II: ~30-50% (Early efficacy signals/dose finding falters)
Phase II to Phase III: ~30-40% (Insufficient efficacy/safety in target populations)
Phase III to Approval: ~50-60% (Pivotal trial failures)
Data from: "The Current Status of Drug Discovery and Development as Originated in United States Academia," PMC6226120
Why Do So Many Promising Candidates Perish in the Valley?
The reasons for this high failure rate are multifaceted, creating a formidable barrier to delivering treatments:
Translational Failures & Preclinical Model Limitations: A primary culprit is the often-poor predictive validity of preclinical models. Animal models, while invaluable, may not accurately replicate the complexity of human diseases or drug responses. As noted by Frontiers in Systems Biology, "The location of the Valley of Death...is evidence that the main problem is...the inability to efficiently translate basic science knowledge obtained from preclinical studies into effective therapies."2 This leads to candidates failing to show efficacy or exhibiting unexpected toxicity in humans.
Insufficient Understanding of Disease Heterogeneity & Target Engagement: Diseases, particularly complex ones like cancer or neurodegenerative disorders, are not monolithic. A drug target validated in a specific cellular context may not be relevant across diverse patient populations or disease subtypes. Failure to demonstrate clear target engagement and a corresponding biological effect in early clinical studies is a common pitfall.
The Funding Chasm: Early-stage clinical development is expensive, and the associated risks are high. Securing adequate, sustained funding to navigate Phase I and II trials, especially for smaller biotechs or academic-led projects, is a significant challenge. This "financial gap" can prematurely terminate promising, albeit high-risk, programs. ResearchGate highlights financial gaps as a primary driver of the VoD.
Suboptimal Clinical Trial Design & Execution:
Poor patient selection or stratification: Enrolling an "all-comers" population when a drug is likely to benefit a specific, molecularly defined subgroup can dilute efficacy signals.
Inappropriate endpoints: Chosen endpoints may not be sensitive enough, clinically relevant, or capture the true patient benefit.
Operational complexities, including issues with site selection, patient recruitment, and data quality, can compromise trial integrity. WCG Clinical notes that "Poor study design is the number one reason for trial failure."
Regulatory Hurdles & Evolving Standards: Navigating the complex regulatory landscape requires significant expertise and resources. Uncertainty about regulatory expectations, especially for novel modalities or endpoints, can deter investment and slow progress.
Lack of Robust Biomarkers: Predictive and pharmacodynamic biomarkers are crucial for identifying responsive patient populations, demonstrating target engagement, and providing early indicators of efficacy. The absence of validated biomarkers significantly increases the risk of failure in later, more expensive phases.
The impact on patients is direct and devastating. Each failure in the valley means delayed access to potentially life-saving or life-improving therapies, continued suffering, and lost hope. As IQVIA points out, "When trials get shut down...patients lose the hope of potentially lifesaving treatments coming to market."
What can be done about this?
While the challenges are immense, we are not without strategies. A multi-pronged, patient-centric approach is essential:
Enhancing Translational Science & Preclinical Rigor:
Improved Models: Investing in more physiologically relevant preclinical models, including humanized mice, patient-derived xenografts (PDXs), organoids, and microphysiological systems ("organs-on-chips"). The NIH's National Center for Advancing Translational Sciences (NCATS) emphasizes that a "major focus of translational science" must be on improving the preclinical to clinical transition.
Reverse Translation: Feeding clinical observations back into preclinical research to refine models and hypotheses.
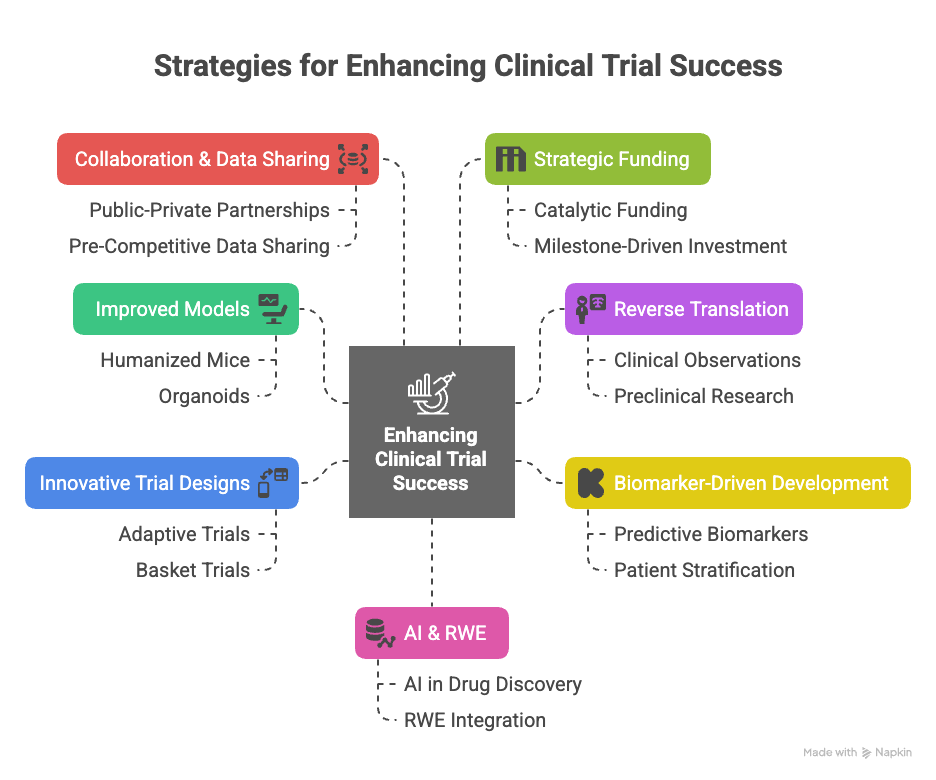
Embracing Biomarker-Driven Development:
Early Integration: Prioritizing the discovery, validation, and integration of predictive, prognostic, pharmacodynamic, and safety biomarkers from the earliest stages.
Patient Stratification: Using validated biomarkers to enrich trial populations for likely responders, increasing the probability of demonstrating efficacy and ensuring the right patients receive the right investigational medicine. This is key to "advancing personalized medicine," as highlighted by research in the European Journal of Public Health.
Innovative and Adaptive Clinical Trial Designs:
Adaptive Trials: Designs that allow for pre-specified modifications based on accumulating data (e.g., sample size re-estimation, arm dropping, population enrichment). The FDA has acknowledged the advantages of such designs for improving statistical efficiency.
Basket/Umbrella/Platform Trials: Efficiently testing multiple drugs in a single disease or a single drug in multiple diseases/molecular subtypes, often under a master protocol.
Fostering Collaboration and Data Sharing:
Public-Private Partnerships: Encouraging collaboration between academia, industry, regulatory agencies, and patient advocacy groups to share knowledge, resources, and risk.
Pre-Competitive Data Sharing: Initiatives that allow for the sharing of baseline data, natural history information, and even anonymized failed trial data can inform future development.
Strategic Funding and De-Risking Initiatives:
Catalytic Funding: Increased availability of grants and venture philanthropy for early, high-risk clinical stages. Organizations like the Rainwater Charitable Foundation exemplify how targeted funding can push therapies forward.
Milestone-Driven Investment: Staging investments based on the achievement of clear translational and clinical milestones.
Leveraging AI and Real-World Evidence (RWE):
AI in Drug Discovery & Development: Utilizing AI for target identification, predicting drug efficacy/toxicity, optimizing trial design, and analyzing complex datasets.
RWE Integration: Using real-world data to inform trial design, identify unmet needs, and understand long-term effectiveness and safety, potentially supplementing traditional trial data where appropriate.
Cautious Optimism for Patients
The "Valley of Death" in clinical development remains a formidable obstacle. However, by embracing scientific rigor, innovative methodologies, collaborative frameworks, and an unwavering focus on the patient, we can improve the odds. It requires a shift from isolated efforts to an integrated ecosystem dedicated to translating scientific promise into clinical reality.
The ultimate beneficiaries of navigating this valley more effectively are the patients whose lives depend on our ability to deliver safe and effective new treatments. The journey is arduous, but the destination—ameliorating human suffering—is a powerful impetus for continued innovation and perseverance.