
CAR-T for Autoimmune Disease: A Safety Reckoning Is Coming – and the Field Is Not Ready
Part 1

I have been monitoring the CAR-T-for-autoimmunity field with growing concern. Not because the science is bad — some of the early lupus data from Erlangen is genuinely remarkable — but because I have seen this movie before. Multiple times. And it doesn’t end well for the patients who need these therapies most.
Let me explain.
The Numbers Don’t Support the Enthusiasm
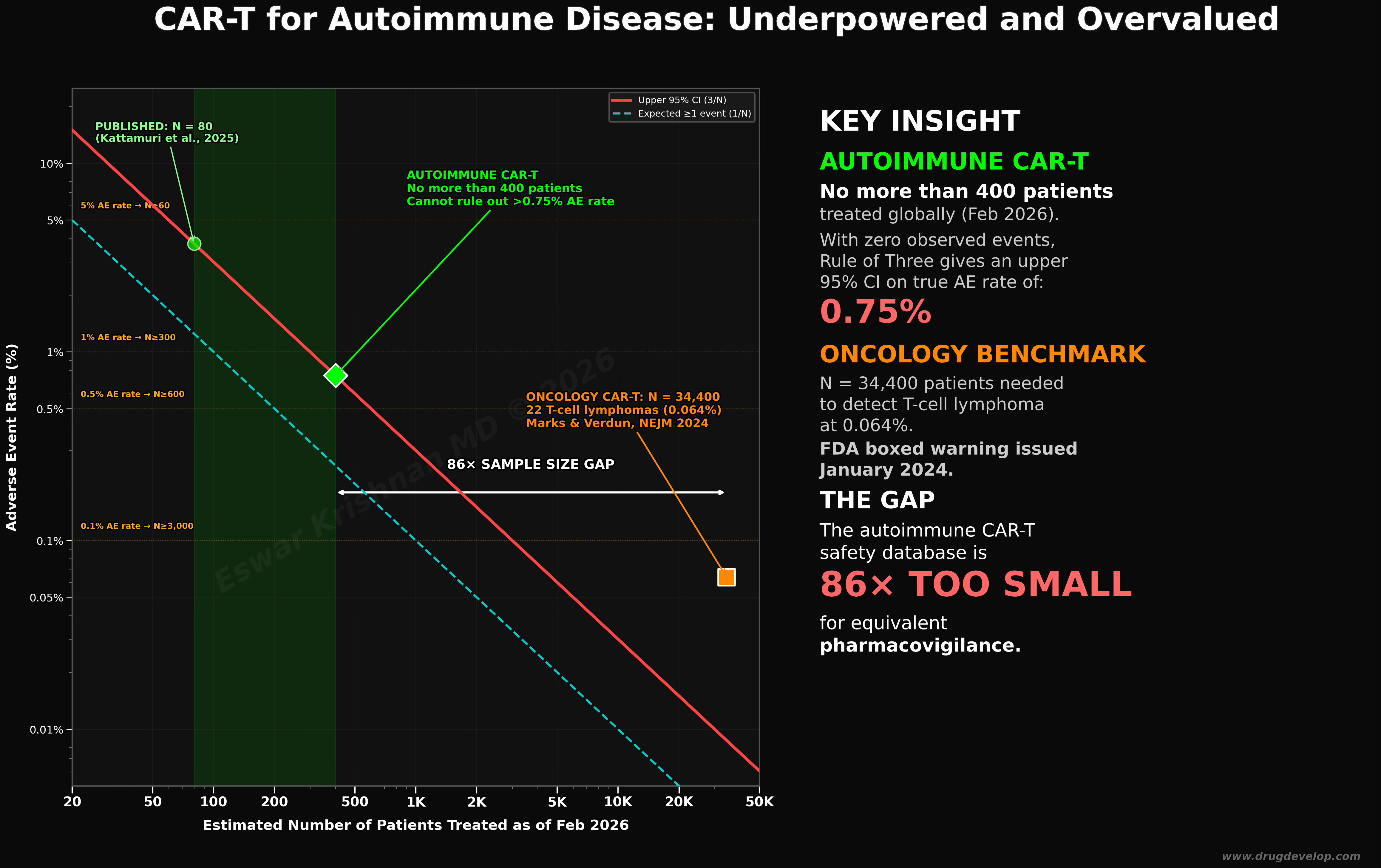
As of February 2026, fewer than 400 patients worldwide have received CAR-T therapy for autoimmune conditions (my optimistic estimate). The published, peer-reviewed literature as of 2024 comprised approximately 80 patients across 24 studies (Kattamuri et al., Rheumatol Int, 2025). Eighty. That is not a typo.
Using the Rule of Three — a standard biostatistical method published in JAMA (Hanley & Lippman-Hand, 1983) — if zero serious adverse events are observed in 400 patients, the upper bound of the 95% confidence interval on the true adverse event rate is 0.75%. That means we cannot rule out that up to 3 in every 400 patients could experience a serious, potentially life-threatening complication that simply hasn’t shown up yet.
For context: oncology CAR-T required 34,400 treated patients before the FDA identified 22 cases of secondary T-cell lymphoma — a signal at 0.064% that triggered a boxed warning in January 2024 (Marks & Verdun, NEJM 2024). The autoimmune safety database is 86 times too small for equivalent pharmacovigilance. At current enrollment rates, matching that level of safety surveillance would take 15–20 years. Perhaps longer. Perhaps never.
We are flying blind.
Too Many Products, No Market Consolidation — We’ve Seen This Before
Currently, there are more than 100 registered clinical trials of CAR-T for autoimmune diseases (Frontiers systematic review, 2025). Over a dozen companies are developing competing constructs targeting CD19, BCMA, or dual targets, each with slightly different manufacturing processes, conditioning regimens, and vector designs. The fragmentation is staggering.
History tells us what happens next.
In the early 1980s, there were dozens of personal computer manufacturers — Commodore, Atari, Tandy, Osborne, Kaypro, and IBM clones by the hundreds. The market consolidated brutally. Microsoft and Intel survived. Most did not. The technology was transformative, but the companies were largely destroyed.
Smartphones followed the same arc. Remember Palm, BlackBerry, Windows Phone, Symbian, WebOS? By 2013, Apple and Android accounted for more than 95% of the market. The underlying technology thrived. The business landscape was a graveyard.
Henry Ford didn’t invent the automobile. He survived the consolidation of more than 250 American car companies between 1900 and 1920. By 1930, three companies controlled 75% of the U.S. market.
The pattern is iron-clad: transformative technology → irrational proliferation → brutal consolidation → a few winners, many casualties. CAR-T for autoimmunity is deep in phase two. The question is not whether consolidation will happen, but how many patients will be mid-treatment when it does.
The “Dumb Capital” Problem
Between 2021 and 2025, cell therapy startups collectively raised more than $15 billion through venture capital and public offerings. Much of this money was not invested by groups with deep immunology expertise or realistic timelines. It was speculative capital chasing the next platform story — the same capital that inflated and then abandoned gene therapy, microbiome therapeutics, and digital health before that.
When this bubble pops — and the Rule of Three analysis above suggests the safety reckoning is a matter of when, not if— the collateral damage will extend far beyond the companies that fail. The entire cell therapy ecosystem will suffer. Investors will retreat. Regulatory scrutiny will intensify. And the patients with refractory lupus, systemic sclerosis, or myositis who desperately need these treatments will find themselves stranded.
We observed precisely this in the field of gene therapy following the death of Jesse Gelsinger in 1999. It took nearly 15 years for clinical gene therapy to recover. Fifteen years of patients waiting because one preventable catastrophe poisoned the well.
“But What About the Alternatives?”
Some colleagues point to emerging competitors—bispecific antibodies, CD19-targeting monoclonals, CAR-NK cells, and in vivo CAR approaches—as evidence that the field will be fine even if autologous CAR-T cells stumble. They argue these alternatives are cheaper, more scalable, and avoid the manufacturing bottleneck.
They are not wrong about the short-term advantages. Bispecific T-cell engagers don’t require leukapheresis, clean-room manufacturing, or a two-week wait. They cost a fraction of the cost of CAR-T. For a budget-constrained rheumatology market, that is a compelling pitch.
But here is what the “alternatives will save us” argument misses: if a safety signal emerges in CAR-T — particularly one involving T-cell malignancy or delayed autoimmune flare — it will not be contained to CAR-T alone. The regulatory and public perception fallout will splash across every therapy that involves engineered immune cell activation. The FDA will not distinguish between CAR-T and CAR-NK when a CNN headline reads “Cancer Therapy Turns Deadly in Lupus Patients.” Fair or not, that is how it works.
My prediction from two years ago still holds: without rigorous, adequately powered safety monitoring — a proper pharmacovigilance infrastructure built before the crisis, not after — this field is heading for a correction that will hurt everyone. Patients. Investors. Developers. The science itself.
So, What Should We Do?
I have specific, actionable recommendations. A unified safety registry. Bayesian adaptive monitoring frameworks. Minimum reporting standards. A realistic conversation about what 400 patients can and cannot tell us. And a framework for how investors should evaluate safety risk—not just efficacy upside—in their due diligence.
But that is Part 2.
Coming soon.
Eswar Krishnan, MD | www.drugdevelop.com
Data sources: Hanley & Lippman-Hand, JAMA 1983; Kattamuri et al., Rheumatol Int 2025; Mueller et al., ASH 2024; Marks & Verdun, NEJM Jan 2024.
#CARTtherapy #CellTherapy #Autoimmune #Pharmacovigilance #DrugSafety #Biostatistics #ClinicalTrials #Rheumatology #Lupus #DrugDevelopment #BiotechInvesting #VentureCapital