
Big Eaters of Immune System: New Therapeutic Targets for Heart Disease
New insights into cardiac macrophage functions are revealing pathways for therapeutic intervention.

Deep within the human heart, immune cells known as macrophages stand guard. Their name means "big eaters," but they are more than simple scavengers. They are key players in heart health, comprising nearly 10% of non-muscle cells in a healthy heart, and their numbers surge during disease.1 Cardiac macrophages exhibit a "Jekyll and Hyde" nature; they can protect by repairing damage or become destructive, worsening inflammation and cardiac issues. Their abundance impacts heart function and stress responses. Scientists are rapidly uncovering the secrets of these macrophages, leading to innovative treatments for challenging heart conditions, offering hope.
The Two Sides of the Coin: Cardiac Macrophage Identities
Cardiac macrophages are not a monolithic population. They come in at least two main "flavors," distinguished by their origins and the presence of a key cell surface marker called CC-motif chemokine receptor 2 (CCR2).1 This fundamental distinction is crucial because it dictates their primary functions and how they might be therapeutically approached.
FIGURE 1. M1 and M2 Macrophages
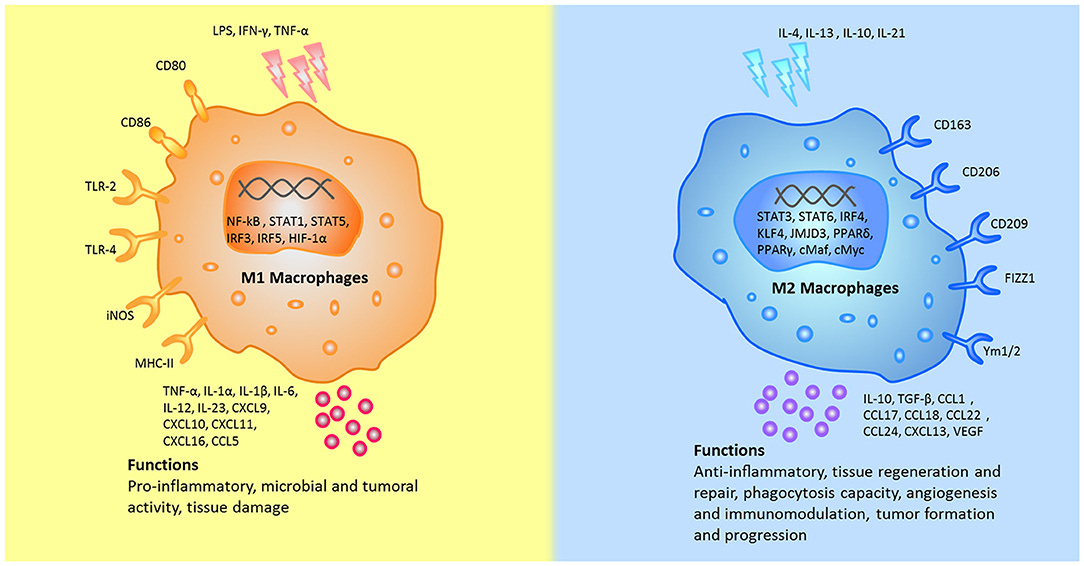
The different stumili, surface markers, secreted cytokines, and biological functions between M1 and M2 macrophages were summarized. CCL, chemokine (C-C motif) ligand; cMaf, c-musculoaponeurotic fibrosarconna; CXCL, chemokine (C-X-C) ligand; FIZZ1, resistin-like α; HIF, hypoxia inducible factor; iNOS, inducible nitric oxide synthase; IFN-γ, interferon-gamma; IL, interleukin; IRF, interferon regulatory factor; JMJD, Jumonji doman-containing protein; KLF, Kruppel-like factor; NF-κB, nuclear factor κB; KLF, Kruppel-like factor; LPS, lipopolysaccharides; MHC, major histocompatibility complex; PPAR, peroxisome proliferator-activated receptors; STAT, signal transducer and activator of transcription; TLR, Toll-like receptor; TNF-α, tumor necrosis factor alpha; TGF-β, transforming growth factor beta; VEGF, vascular endothelial growth factor; Ym1, chitinase 3-like 3.
The first type, embryo-derived CCR2-macrophages, can be thought of as the heart's "resident peacekeepers" or "master builders." Originating early in development, these cells are long-lived and self-renewing, residing within the heart tissue for extended periods.1 Their primary responsibilities include overseeing normal heart development, performing routine maintenance, orchestrating tissue repair, promoting the growth of new blood vessels (angiogenesis), and efficiently clearing cellular debris through a process called efferocytosis.1 Generally, these CCR2- macrophages are considered the "good guys," essential for maintaining a healthy cardiac environment.
In contrast, monocyte-derived CCR2+ macrophages are the "recruited reinforcements." These cells originate from precursors in the bone marrow, circulate in the blood as monocytes, and are rapidly summoned to the heart in response to injury or inflammation.1 Once at the site of trouble, they often adopt a pro-inflammatory stance, releasing substances that can contribute to further tissue damage, promote scarring (fibrosis), and generally exacerbate the underlying disease.1
This CCR2- versus CCR2+ classification isn’t just a concept confined to laboratory models; it also holds significant relevance for the human heart. The unique origins and maintenance mechanisms of these two cell populations—self-renewing CCR2- cells and continuously replaced CCR2+ cells—suggest that we can develop therapeutic strategies with enhanced specificity. For example, we might find ways to reduce the harmful influx of CCR2+ macrophages while preserving the beneficial resident CCR2- population. Moreover, innovative methods like single-cell RNA sequencing are uncovering even more diversity within these broad categories, helping us identify new macrophage subsets and states that can appear during disease. This ongoing refinement of our understanding of macrophage identity is unveiling a wealth of exciting potential new therapeutic targets.
Meet the Macrophage Duo!
CCR2- Macrophages (The Builders & Peacekeepers):
Origin: Embryonic
Residence: Tissue-resident in the heart
Primary Roles: Heart development, routine maintenance, tissue repair, angiogenesis, debris clearance (efferocytosis)
General Impact: Mostly protective and essential for homeostasis 1
CCR2+ Macrophages (The Fighters & Reinforcements):
Origin: Monocyte-derived (from bone marrow via blood)
Residence: Recruited to the heart during injury/inflammation
Primary Roles: Often pro-inflammatory, involved in acute immune responses
General Impact: Can contribute to tissue damage and disease progression if uncontrolled 1
Macrophages in the Line of Fire: Key Cardiac Conditions
The balance and behavior of these macrophage populations shift dramatically in various cardiac diseases, often determining the course and severity of the condition.
Myocardial Infarction and Macrophages: A Double-Edged Sword
Following a myocardial infarction (MI), or heart attack, the role of macrophages is marked by dramatic entrances and shifting functions. Dying heart cells release "danger signals"—damage-associated molecular patterns (DAMPs)—that act like an emergency beacon, summoning CCR2+ monocytes from the blood to the injured area. These early-arriving monocyte-derived macrophages differentiate and unleash a barrage of inflammatory substances, including cytokines like interleukin-1β (IL−1β) and interleukin-6 (IL-6), as well as chemokines such as CXCL2 and CXCL5. While this inflammatory response is part of the body's effort to clear debris and initiate healing, it can also cause significant collateral damage to the surrounding heart tissue and recruit even more inflammatory cells, such as neutrophils, thereby contributing to adverse cardiac remodeling—changes in the heart's size, shape, and function that can lead to heart failure.
Nevertheless, the role of macrophages in myocardial infarction (MI) extends beyond mere destruction. Once the initial inflammatory response diminishes, macrophages—especially the resident CCR2- type and possibly some CCR2+ macrophages that alter their function—become essential for healing and repair. A vital function they perform is efferocytosis, which is the effective engulfment and elimination of dead cells and cellular debris.
This cleanup operation, often mediated by receptors like MERTK on macrophages, is not merely passive "garbage collection"; it's an active process that sends signals to promote the resolution of inflammation and initiate tissue repair. This includes the formation of new lymphatic vessels (lymphangiogenesis), which help drain fluid and immune cells from the injured area.
Understanding the temporal dynamics of the macrophage response—initial pro-inflammatory activity followed by a later pro-reparative phase—is essential. This biphasic characteristic highlights the importance of timing when considering macrophage-targeted therapies for myocardial infarction (MI), ensuring that these interventions facilitate rather than obstruct the healing process. Additionally, recent studies have uncovered specialized subsets of macrophages that emerge after myocardial infarction (MI), including TREM2-High macrophages, which are involved in clearing apoptotic cells, and reparative Vegfb-expressing macrophages, underscoring the complexity of the macrophage response.
It's increasingly clear that recruited cardiac macrophages likely exist in a continuum of states, adapting their function based on the evolving microenvironment of the healing heart.
Heart Failure: A Chronic Battle Involving Macrophages
In chronic heart failure, a condition in which the heart cannot pump blood effectively, macrophages contribute to a state of persistent, low-grade inflammation and play a key role in the development of cardiac fibrosis.1 Fibrosis is the excessive scarring of heart tissue. While some scar formation is necessary to repair areas damaged by injury (such as a myocardial infarction, or MI), excessive fibrosis makes the heart muscle stiff and less compliant, impairing its ability to both pump blood out (systolic dysfunction) and fill with blood adequately (diastolic dysfunction).1
Macrophages fuel the detrimental scarring process in the heart by releasing a variety of signaling molecules that directly activate cardiac fibroblasts—the cells responsible for producing scar tissue. Key among these macrophage-derived mediators are Transforming Growth Factor-beta (TGFβ) and Osteopontin (also known as SPP1).
Studies using advanced imaging techniques have shown that SPP1-expressing macrophages often cluster with activated fibroblasts in fibrotic regions of the heart. This suggests intense, localized communication between these cell types. The crosstalk between macrophages and fibroblasts represents a critical pathogenic axis in heart failure.
Adding another layer of complexity, some research suggests that macrophages themselves might transition and adopt a fibroblast-like phenotype. This transition could directly contribute to the pool of scar-producing cells.
Recent studies have also identified specific pro-fibrotic macrophage subsets, such as CD206+IL-4Rα+ macrophages. These subsets expand in heart failure and secrete proteins, such as FIZZ1, that drive pathological remodeling.
Understanding and interrupting these cellular conversations and transformations holds significant promise for developing anti-fibrotic therapies.
Myocarditis: When Inflammation Attacks the Heart Muscle
Myocarditis is characterized by direct inflammation of the heart muscle (myocardium), and macrophages play a key role in this inflammatory process. A particularly challenging form is immune checkpoint inhibitor (ICI)-induced myocarditis, a potentially life-threatening side effect that can arise in cancer patients undergoing these powerful immunotherapies.
In ICI-induced myocarditis, a specific population of CCR2+ cardiac macrophages that express the chemokines CXCL9 and CXCL10 is found to be significantly increased within the heart tissue.1 These macrophages engage in a detrimental crosstalk with T-cells, another type of immune cell. The interaction is often mediated by interferon-gamma (IFNγ), a potent inflammatory signal released by activated T-cells, which in turn stimulates the macrophages to produce more CXCL9 and CXCL10. These chemokines then attract even more T-cells (specifically those expressing the CXCR3 receptor) to the heart, creating a vicious cycle of inflammation.1 The identification of this specific CXCL9/10-expressing macrophage population and the signaling axis it participates in (IFN-gamma- CXCL9/10- CXCR3) is a significant step forward. It not only provides a clearer understanding of how ICI-myocarditis develops but also offers potential diagnostic markers (e.g., detecting these macrophages in biopsies) and highly specific therapeutic targets.1
Atherosclerosis: Macrophages in the Arterial Battlefield
Atherosclerosis, which is the main culprit behind most heart attacks and strokes, is characterized by the slow accumulation of fatty plaques in the artery walls. Macrophages play a crucial role right from the start of this concerning process. It all kicks off when circulating monocytes are invited into the artery wall, where they start to transform into macrophages. These hardworking macrophages eagerly consume modified forms of cholesterol, especially oxidized low-density lipoprotein (oxLDL), using special scavenger receptors like CD36 and SR-A1. As they fill up with lipids, they become "foam cells," a key feature of early atherosclerotic plaques.
These macrophage-derived foam cells are actively involved in the process; they engage metabolically and release a variety of inflammatory signals, such as IL−1β, which can further encourage plaque growth, inflammation, and, in the end, lead to plaque instability, making them more vulnerable to rupture and increasing the risk of acute cardiovascular events.1 The receptor TREM2, which is present on macrophages, has a role in lipid uptake and the survival of foam cells. However, its exact influence can be quite complex, occasionally appearing to promote atherogenesis and at other times potentially stabilizing plaques, which underscores the intricate roles of macrophage pathways.8
A fascinating and relatively recent discovery links atherosclerosis to an age-related phenomenon called Clonal Hematopoiesis of Indeterminate Potential (CHIP). In CHIP, stem cells in the bone marrow acquire certain genetic mutations (e.g., in the TET2 gene) and give rise to an expanded lineage of blood cells, including macrophages.1 If these macrophages inherit a CHIP-associated mutation like one in TET2, they can become hyper-inflammatory, overproducing IL−1β via the NLRP3 inflammasome pathway, which significantly accelerates the development and progression of atherosclerosis.1 This discovery connects systemic aging processes in the bone marrow directly to cardiovascular disease through specific macrophage dysfunctions, opening new avenues for risk assessment and targeted therapies.
Turning the Tide: Exciting New Treatments Targeting Macrophages
The exciting news is that our deeper understanding of cardiac macrophage biology is sparking a revolution in treatment strategies! Scientists are moving beyond just broadly suppressing inflammation and are instead focusing on developing much more sophisticated and targeted approaches. It’s wonderful to see this evolution: from those early attempts with broad cytokine blockade to the highly specific targeting of pathways, and now even to uniquely identifying distinct cell populations and their special characteristics.
Neutralizing Harmful Signals – Silencing the Inflammation
One major strategy involves directly neutralizing the harmful inflammatory signals produced by or activating macrophages.
Cytokine Inhibitors: Antibodies targeting specific cytokines have shown considerable promise. For example, Canakinumab, an antibody against IL−1β, has been shown in large clinical trials to reduce major adverse cardiovascular events and heart failure-related hospitalizations in high-risk patients.1 Rilonacept, another IL−1β blocker, is effective for recurrent pericarditis.1 Similarly, inhibitors of the IL-6 receptor have demonstrated benefits in improving myocardial salvage after a heart attack.1 The limited success of broader agents like TNF inhibitors in some cardiac conditions underscores that specificity is key.1
NLRP3 Inflammasome Inhibitors: Since the NLRP3 inflammasome is a critical intracellular complex required for the processing and release of active IL−1β and IL-18, its inhibitors are being actively investigated.1 These hold particular promise for conditions like CHIP-driven atherosclerosis, where NLRP3 activation in macrophages is a key pathogenic step, and clinical trials are underway.1
Controlling Macrophage Traffic – Managing the Crowd
Another approach is to control the recruitment of detrimental macrophage populations to the heart.
CCL17 Inhibition: The chemokine CCL17, produced mainly by CCR2+ macrophages, can suppress the recruitment of beneficial regulatory T-cells to the injured heart. Blocking CCL17 in animal models has been shown to boost regulatory T-cell numbers, reduce inflammation, and limit adverse cardiac remodeling.1
CXCR3-CXCL9/10 Axis Blockade: As mentioned in the context of ICI-myocarditis, disrupting the interaction between macrophage-derived CXCL9/10 and the CXCR3 receptor on T-cells is a promising therapeutic strategy for this specific condition, aiming to break the inflammatory feedback loop.1
Precision Strikes – Targeting Specific Villains or Boosting Heroes
The most exciting frontier involves highly precise interventions, either by selectively targeting detrimental macrophage subsets or by actively promoting the functions of beneficial ones. This includes strategies for "re-educating" or reprogramming macrophages.
Targeting Pro-Fibrotic Macrophages in Heart Failure: Research is focusing on ways to specifically inhibit pro-fibrotic macrophage populations, such as the CD206+ IL-4R-alpha+ macrophages that produce FIZZ1. Modulating IL-4R-alpha signaling on these cells is being explored to reduce cardiac fibrosis and improve heart function.3
Re-educating Macrophages in Atherosclerosis:
Unc5b Deletion: Preclinical studies demonstrate that deleting the Unc5b receptor specifically in myeloid cells can reduce atherosclerotic plaque burden and promote a more pro-resolving immune environment within advanced plaques.9
UDP-003 (Cyclarity Therapeutics): This investigational drug is designed to specifically remove 7-ketocholesterol, a toxic form of oxidized cholesterol, from foam cells. The goal is to revert these lipid-laden macrophages back into healthy, functional cells capable of clearing plaque. UDP-003 is currently in Phase 1 clinical trials, representing a novel "macrophage re-education" strategy.11
Nanomaterial-based therapies: Tiny, engineered particles are being developed to deliver drugs directly to atherosclerotic plaques, clearing foam cells, reducing local inflammation, or promoting plaque stabilization.13
Boosting Reparative Functions Post-MI:
Endothelial HSPA12B Exosomes: Exosomes (tiny vesicles released by cells) derived from endothelial cells expressing Heat Shock Protein A12B (HSPA12B) have been found to promote the polarization of macrophages towards a beneficial M2 (pro-regenerative) phenotype and suppress harmful TLR4/MyD88 signaling after MI.14
M2 Macrophage-Derived Exosomes (M2-Exos): Similarly, exosomes harvested from M2 macrophages are being explored for their therapeutic potential, as they can deliver a cargo of anti-inflammatory and pro-angiogenic molecules to injured tissues.15
CAR-Macrophage Therapy: This cutting-edge "living therapy" involves genetically engineering a patient's own macrophages to recognize and attack specific targets. For example, Fibroblast Activation Protein (FAP) CAR-macrophages are designed to target FAP-expressing activated fibroblasts in areas of cardiac fibrosis. Preclinical studies have demonstrated that these FAP CAR-Ms can reduce fibrosis and enhance heart function following ischemia-reperfusion injury, highlighting their potential to reprogram immune cells for direct therapeutic action.16
The emergence of such sophisticated strategies, which move beyond simple suppression to nuanced modulation and cellular engineering, signifies a paradigm shift in how cardiac diseases are treated.
Callout Box: Healing Hearts: The Next Wave of Treatments!
Cytokine Blockers: Cooling down the inflammatory fire by neutralizing specific signals like IL−1β or IL-6.1
Macrophage Re-education: Turning harmful foam cells back into helpful macrophages (e.g., UDP-003 for atherosclerosis).11
CAR-Macrophages: Engineering "super-powered" macrophages to target and eliminate disease-promoting cells like activated fibroblasts.17
Exosome Therapy: Using tiny vesicles released by cells to deliver healing messages and molecules to the injured heart.14
Conclusion: A Hopeful Horizon for Heart Health
Macrophages are powerful, multifaceted cells in the cardiac ecosystem, acting as a double-edged sword in both cardiac disease and repair. Recent advancements, such as single-cell sequencing, reveal new macrophage subsets and their unique functions. This ongoing discovery expands potential therapeutic targets. Many macrophage-targeted therapies are still in preclinical development or early trials, yet the progress is exciting. Targeting specific macrophage populations or reprogramming their behavior offers immense hope. A key challenge will be translating preclinical findings into safe and effective therapies for humans, which requires robust clinical trial data, personalized approaches, and sophisticated drug delivery systems. With ongoing research and promising new strategies, the future of utilizing macrophages to treat heart disease looks promising, making these immune system titans likely allies in promoting long-term heart health.
Works cited
Yang, S., Penna, V. & Lavine, K.J. Functional diversity of cardiac macrophages in health and disease. Nat Rev Cardiol 22, 431–442 (2025). https://doi.org/10.1038/s41569-024-01109-8
Transition of Macrophages to Fibroblast-Like Cells in Healing Myocardial Infarction - JACC, accessed May 29, 2025, https://www.jacc.org/doi/abs/10.1016/j.jacc.2019.10.036
CD206+IL-4Rα+ Macrophages Are Drivers of Adverse Cardiac ..., accessed May 29, 2025, https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.124.072411
CD206+IL-4Ralpha+ MACROPHAGES ARE DRIVERS OF ..., accessed May 29, 2025, https://www.researchgate.net/publication/384610908_CD206IL-4Ralpha_MACROPHAGES_ARE_DRIVERS_OF_ADVERSE_CARDIAC_REMODELING_IN_ISCHEMIC_CARDIOMYOPATHY
CD206+IL-4Rα+ MACROPHAGES ARE DRIVERS OF ADVERSE CARDIAC REMODELING IN ISCHEMIC CARDIOMYOPATHY | medRxiv, accessed May 29, 2025, https://www.medrxiv.org/content/10.1101/2024.10.01.24314741v1
Novel Therapeutic Approach Targeting CXCR3 to Treat Immunotherapy Myocarditis | Circulation Research - American Heart Association Journals, accessed May 29, 2025, https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.124.325652
Novel Therapeutic Approach Targeting CXCR3 to Treat Immunotherapy Myocarditis, accessed May 29, 2025, https://pubmed.ncbi.nlm.nih.gov/39931812/
Foamy macrophages in atherosclerosis: unraveling the balance ..., accessed May 29, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC12081418/
Targeting Unc5b in macrophages drives atherosclerosis regression and pro-resolving immune cell function | PNAS, accessed May 29, 2025, https://www.pnas.org/doi/10.1073/pnas.2412690121
Targeting Unc5b in macrophages drives atherosclerosis regression and pro-resolving immune cell function - PubMed, accessed May 29, 2025, https://pubmed.ncbi.nlm.nih.gov/39436659/
Cyclarity Therapeutics Launches First-in-Human Trial of UDP-003 for Atherosclerosis, accessed May 29, 2025, https://trial.medpath.com/news/574b66f5a925a0c2/news-for-the-cardiac-and-vascular-medtech-and-biotech
Our Science - Cyclarity Therapeutics, accessed May 29, 2025, https://cyclaritytx.com/our-science/
Full article: Advances in the treatment of atherosclerotic plaque ..., accessed May 29, 2025, https://www.tandfonline.com/doi/full/10.1080/17435889.2025.2480049?src=
Endothelial HSPA12B regulates myocardial monocyte ... - Frontiers, accessed May 29, 2025, https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2025.1587898/full
Macrophage-driven exosomes regulate the progression ... - Frontiers, accessed May 29, 2025, https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2025.1563800/full
CAR-Macrophage Therapy Alleviates Myocardial Ischemia-Reperfusion Injury | Circulation Research - American Heart Association Journals, accessed May 29, 2025, https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.124.325212
CAR-Macrophage Therapy Alleviates Myocardial Ischemia ..., accessed May 29, 2025, https://www.ahajournals.org/doi/abs/10.1161/CIRCRESAHA.124.325212
CAR-Macrophage Therapy Alleviates Myocardial Ischemia-Reperfusion Injury - PubMed, accessed May 29, 2025, https://pubmed.ncbi.nlm.nih.gov/39465245/